
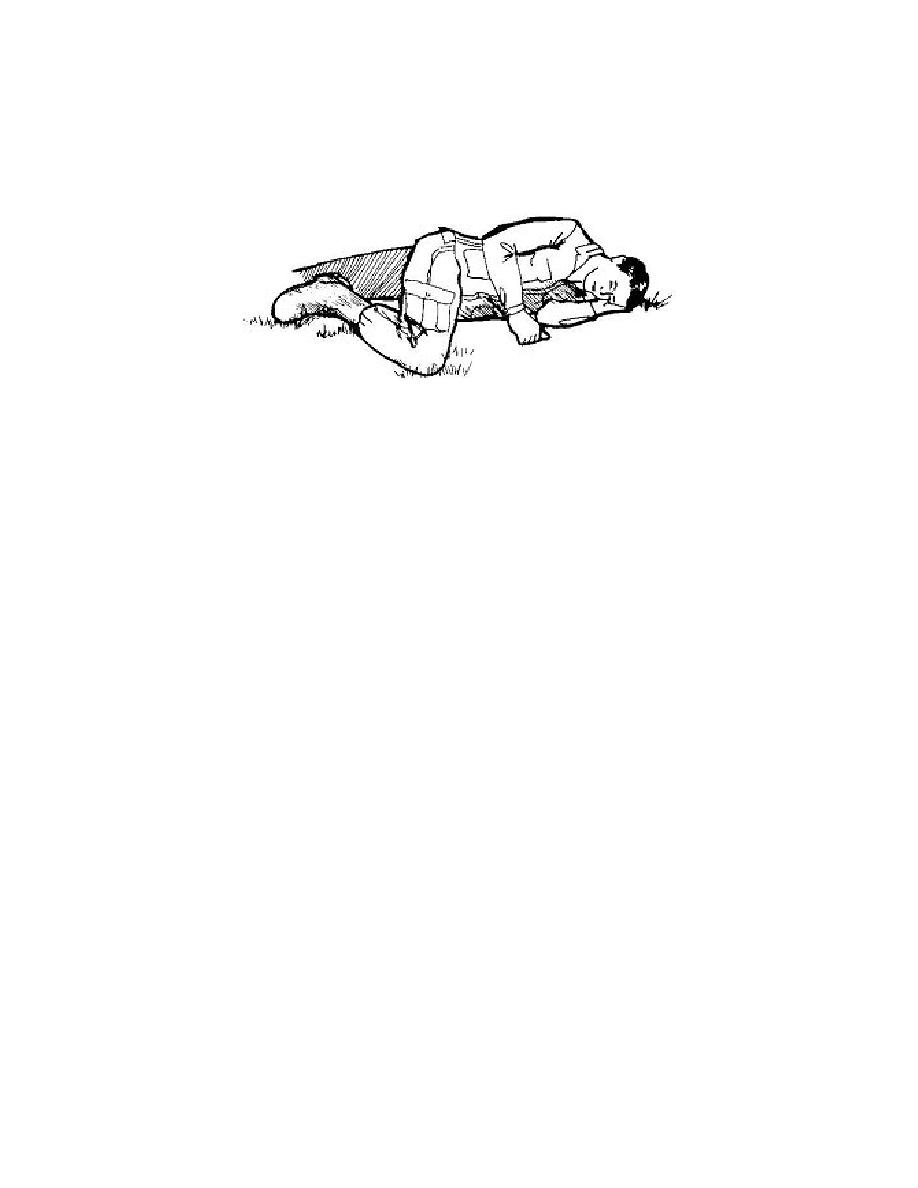
(d) If the casualty has no additional injuries, roll the casualty into the
recovery position (on his side). This allows for accumulated blood and mucus to drain
from the casualty's mouth instead of choking the casualty. See figure 1-1.
Figure 1-1. Unconscious casualty placed in the recovery position.
e. Chest. Assess and treat the casualty for chest injuries (Lesson 4).
(1) Expose the chest and check for equal rise and fall. Remove the
minimum of clothing required to expose and treat injuries. Protect the casualty from the
environment (heat and cold) as much as possible.
(2) Examine the chest for wounds. Check for both entrance and exit
wounds (sucking chest wounds).
(3) Immediately seal any penetrating injuries to the chest with airtight
material. Seal one open chest wound with a three-sided seal (one side of airtight
material left untaped). Sealing the wound keeps air from entering the wound. If air can
freely enter through the wound, the casualty's lung may collapse. The three-sided seal
prevents air from entering the chest, but allows trapped air to escape.
(4) Monitor the casualty for progressive severe respiratory distress
(breathing becomes more labored and faster). If respiration becomes progressively
worse, assume tension pneumothorax exists and decompress the affected chest side
with a 14-gauge needle inserted at second intercostal space (ICS) on mid-clavicular line
(MCL). Secure the catheter in place with tape.
CAUTION:
Only perform needle chest decompression on a casualty with a
penetrating (sucking) chest wound.
(5) If the casualty has been treated for an open chest wound, position or
transport the casualty with the affected side down, if possible. The body pressure acts
to "splint" the affected side.
IS0871
1-6

 Previous Page
Previous Page
